

Including nursing home residents in a general population health survey in Germany
Gaertner B., Koschollek C., Grube M.M., Lüdtke D., Fuchs J., Scheidt-Nave C. et al. (2019). Including nursing home residents in a general population health survey in Germany. Survey Methods: Insights from the Field. Retrieved from https://surveyinsights.org/?p=10807
© the authors 2019. This work is licensed under a Creative Commons Attribution 4.0 International License (CC BY 4.0) 
Abstract
Nursing home residents (NHRs) are systematically excluded from the target populations of most population-based health surveys, which may result in biased prevalence estimates. Researchers who wish to include NHRs in surveys face several challenges including difficulty sampling and contacting NHRs and greater levels of functional impairments impeding participation. A population-wide, register-based, random sample of 8,000 older individuals (57.1% women, mean age=76.2 years) in six primary sampling units (PSUs) in Germany was used to analyse NHR coverage. The contact and response rates among NHRs were compared to those among persons living in private households in two PSUs (N=2,000) by applying an informed sequential mixed-mode design. All persons received a health questionnaire by mail, and random subgroups of initial non-respondents were further contacted by telephone or personal visits. The population-wide, register-based, random sample included a substantial proportion of NHRs that nearly approximated the national rate of 4.2% NHRs among individuals ≥65 years. Never-theless, undercoverage of a specific subgroup of NHRs was apparent. The contact and re-sponse rates were significantly lower among NHRs than persons in private households (contact: 49.0% vs. 72.9%; response: 20.0% vs. 45.9%). Therefore, it remains questionable if NHRs can be included in regular national health monitoring programmes.
Keywords
coverage, hard-to-reach, nursing home residents, register-based sampling design, sequential mixed-mode design
Acknowledgement
The authors wish to thank all of our colleagues at the Robert Koch Institute, the staff at the registration offices who supported our study and the study participants as well as their proxies for taking the time to participate. This work was supported by the Robert Bosch foundation (Grant Number: 11.5.G410.0001.0). The contents of this publication are solely the responsibility of the authors.
Copyright
© the authors 2019. This work is licensed under a Creative Commons Attribution 4.0 International License (CC BY 4.0)
Introduction
The proportion of older people in Germany, as in other high-income countries, has been steadily increasing over the past several decades. In Germany, 4.2% of the population 65 years and older and 11.5% of the population 80 years and older are living in a nursing home [1]. However, data on the health status and the health needs of older adults are largely insufficient for those in residential care. This is partly because general population surveys commonly exclude residents of non-private households from their target populations [2]. In addition, age limits of 80 or 85 years are often applied to study eligibility requirements [3, 4].
From an ethical perspective, this exclusion is controversial. Nursing home residents constitute a vulnerable subgroup of the society and, pursuant to the Helsinki Declaration of the World Medical Association [5], should be involved in studies only if “the research is responsive to the health needs or priorities of this group and the research cannot be carried out in a non-vulnerable group” (principle 20). However, this is true only if information is not available from other sources such as routine data.
Since the prevalence of morbidity and functional limitations is higher among nursing home residents than older adults living at home, the exclusion of institutionalized persons from general health surveys can substantially bias survey estimates of health-related outcomes [6, 7]. Analyses from a Swedish study of older adults showed that the estimated prevalence of individuals experiencing three or more limitations in activities of daily living increased from 2.8% for participants living at home who could be directly interviewed to 16.2% when both proxies and institutionalized persons were included in the analyses [7]. Excluding institutionalized persons from general population studies might also lead to an underestimation of social disparities in health [8, 9]. In addition, the proportion of older adults living in institutional care varies across countries and over time. Hence, neglecting this population in health studies is problematic for comparative analyses as well [7, 10].
Even if nursing home residents are not explicitly excluded from study participation, the sampling methods and data collection procedures applied often seem inadequate for reaching older adults living in institutional care. Researchers wishing to include nursing home residents in general population surveys must tackle a range of methodological and practical issues concerning coverage, contactability and participation ability.
With regard to coverage, there is debate concerning whether sampling procedures based on municipal population registers lead to an underrepresentation of older adults living in institutional care in the gross sample [2]. If municipal population registers are based on addresses of households, as in the Netherlands, for example, then the sample probabilities are lowered for the inhabitants of institutions. If municipal registers are based on individuals, as they are in Germany, then the samples drawn from those registers should have fewer problems with undercoverage of nursing home residents. However, some German registration authorities might not provide the addresses of persons living in institutions due to an information release ban, which restricts the release of information on nursing home residents and other institutionalised individuals according to Section 52, Federal Act on Registration (German: “bedingter Sperrvermerk nach § 52 Bundesmeldegesetz”) [11]. According to this regulation, registration authorities are allowed to provide addresses of nursing home residents only to other public authorities. Since the regulation has been in force for only a short period and as registration offices are largely decentralized, it remains unknown to what extent this regulation constrains the coverage of nursing home residents in register-based samples.
A major challenge that researchers of nursing home studies are facing is the increased likelihood of poor health, cognitive impairment and dementia among older adults in institutional care impeding their ability to be interviewed. Previous studies have found that between 30% and 40% of nursing home residents are capable of being interviewed directly, without the assistance of a proxy [6, 7]. Informed consent can also be difficult to obtain or might require the involvement of a legally authorized representative [5, 12]. Other challenges lie in the organisation of the institutional setting itself. Seizing an interview opportunity in between residents’ busy schedules might sometimes prove difficult, as can ensuring privacy during face-to-face interviews [13].
The ability to contact nursing home residents is limited, as they are a specifically vulnerable subgroup of older adults, and both nursing home staff and families often act as gatekeepers who wish to protect them from being contacted for research purposes [12, 14, 15].
In this study, we aimed to assess the coverage of nursing home residents in a random sample based on individual address data from municipal population registers (aim 1). To reach this aim, it was necessary to verify how we can reliably identify nursing home residents relying on individual address data. In addition, we examined the participation, cooperation and contact rates of nursing home residents and compared these values with those of samples from private households (aim 2).
Methods
We report the results from a pilot study on health in older age groups that was conducted as part of the “IMOA – Improving Health Monitoring in Old Age” project, funded by the Robert Bosch Foundation (Grant Number: 11.5.G410.0001.0). The main objectives of the project were (1) to develop a conceptual framework for public health monitoring of the population aged 65 years and older and to select key indicators to monitor health in older populations and (2) to adapt sampling and recruitment strategies according to the needs and capabilities of older adults.
The pilot study was conducted between September 2017 and April 2018 at the Robert Koch Institute Berlin, Germany, a public authority subordinate to the Federal Ministry of Health. The study was approved by the ethics committee at the Berlin Chamber of Physicians (German: “Berliner Ärztekammer”, Eth-22/17) and was conducted in compliance with data protection and privacy regulations, as required by the Federal Commissioner for Data Protection and Freedom of Information. Informed written consent was obtained from all participants who completed a questionnaire or had a face-to-face interview. Oral consent was obtained from participants who had a telephone interview. For proxy participation, written informed consent from the invited individual or his/ her legally authorized representative was required.
Sampling frame and participation
A two-stage sampling approach was used in the study (Figure 1). First, six primary sampling units (PSUs) were selected from the total number of federal municipalities in Germany. The PSUs included an equal number of West and East German municipalities; two PSUs were selected from urban areas (≥100,000 inhabitants), and four PSUs were selected from rural areas (<100,000 inhabitants). Only municipalities with at least one nursing home and at least 1,000 inhabitants 65 years of age and older who lived in the municipality were considered. Second, a random sample of 8,000 individuals 65 years and older with a permanent residence in the sampled communities was drawn proportionally to the overall population from the population registers of the chosen municipalities on September 11, 2017. The drawn numbers differed between PSUs in urban and rural areas (n=2,000 vs. n=1,000, respectively). The total sample (n=8,000) was used to assess the coverage of nursing home residents in the sample (aim 1).
Figure 1. Sample composition

Due to limited resources, subsequent testing of the survey design (aim 2) was restricted to only two PSUs that included 2,000 individuals. The study procedures are described in detail elsewhere [16]. In brief, recruitment for study participation was conducted between October and December 2017 by trained research assistants. All individuals were initially contacted through postal mail, followed by one reminder letter. If no final response was received, individuals were further contacted via telephone (maximum 10 calls, depending on the availability of a telephone number provided by one commercial provider) or personal visits (maximum two visits). Due to limited resources, these staff-intensive recruitment efforts were applied only to random subsamples (telephone group: n=250; home visit group: n=160). Finally, if no contact was achieved after ten telephone calls, individuals in the telephone group additionally received a maximum of two personal visits.
Throughout all recruitment stages, study participation was possible by sending back the completed short health questionnaire or by taking part in a telephone or face-to-face interview. Participation was also possible through proxy-only interviews/questionnaires as well as partly proxy interviews/questionnaires. More details are provided elsewhere [16].
Measures
Register based-information
Register-based information for the total sample (n=8,000) included sex, date of birth, postal addresses and, if applicable, the existence of an information release ban.
In the subsample used for testing the survey design (n=2,000), further register-based information, including marital status and citizenship, was requested from the registration authorities. Marital status was categorised as being married/living in a registered partnership (yes/no), and citizenship was categorised into German vs. non-German.
Identification of nursing home residents
Three independent strategies were used to identify nursing home residents within the total sample. First, individuals assigned an information release ban were assumed to be nursing home residents (“information release ban”, yes/no). Individuals not assigned an information release ban but who were living at an identical postal address as someone with an information release ban were also assumed to be nursing home residents (“living at a ban address”, yes/no). As a second strategy, we used an online database to search for nursing home addresses within the PSUs using postal codes [17]. As an additional step, we searched the internet if a postal address was found at least three times in the data we received from the registration authorities to determine whether it was the postal address of a nursing home (“internet search”, yes/no). Finally (strategy 3), we purchased addresses of nursing homes within the PSUs from a commercial provider (pm pflegemarkt.com GmbH, Hamburg, Germany) (“commercial provider”, yes/no). Nursing home addresses identified by strategies two and three were compared to postal addresses received from the registration authorities. A dichotomised variable indicated if an individual was identified as a nursing home resident at least once (“identification at least once”, yes/no).
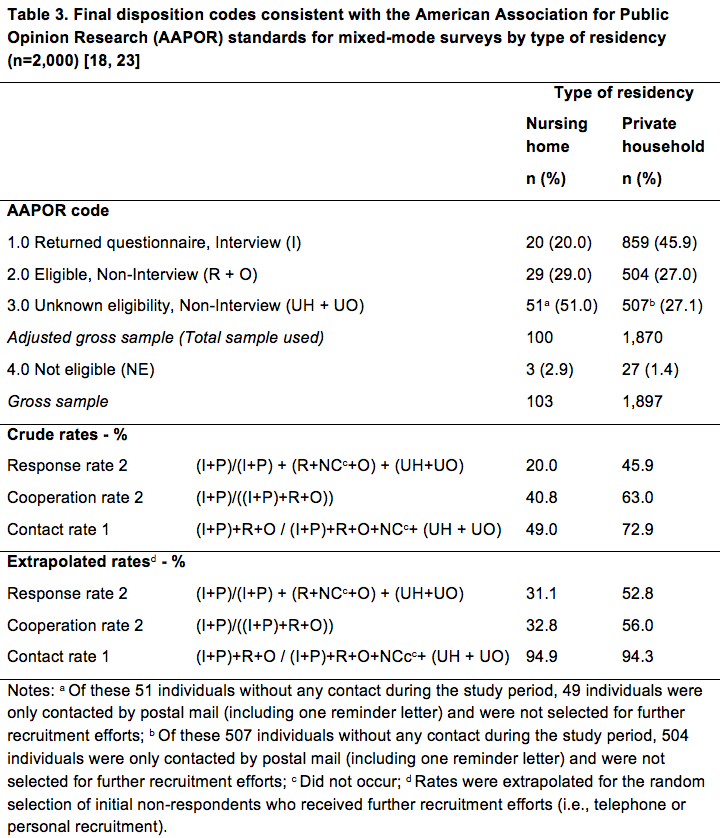
Final disposition codes
Final disposition codes were determined according to the American Association for Public Opinion Research (AAPOR) standards [18]. The final disposition code “interview” was assigned to all completed questionnaires/interviews with ≥80% of the applicable questions answered and for partial questionnaires/interviews with at least 50% of the applicable questions answered. The following cases were defined as an “eligible non-interview”: if the sample person refused an questionnaire/interview, broke off an interview, moved outside of the PSU during the field period, died during the field period, did not provide a decision regarding participation or refusal during a personal contact or did not provide written informed consent or if the questionnaire was lost. The final disposition code “unknown eligibility, non-interview” was assigned when no mailed questionnaires were returned, no contact could be established by phone or personal visit, or nothing was known about the sample person or the address. The final disposition code “not eligible” was assigned to persons outside of the sample frame, namely, individuals who died or moved out of the PSUs before recruitment started and persons without sufficient German language skills.
Statistical Analyses
Descriptive statistics stratified by PSUs were calculated. Then, group differences between nursing home residents and those living in private households were analysed using descriptive and Chi² statistics. Statistical analyses were conducted using Stata/SE 15.1 [19]. P-values less than 0.05 were considered significant. Due to the feasibility character of the study, the complex sampling was not taken into account to adjust standard errors.
Crude response, cooperation and contact rates were calculated according to AAPOR standards [18]; i.e., contact rate 1, cooperation rate 2 and response rate 2. Further recruitment of initial non-respondents was only carried out among random subgroups, i.e. 125 individuals of each PSU with an available telephone number were randomly selected for the telephone group (total: n=250) and 80 individuals of each PSU without an available telephone number were randomly selected for the home visit group (total: n=160). A total of 561 individuals were therefore not selected for further recruitments efforts. An extrapolation factor was calculated that considered this disproportionate selection probability dependent on PSUs and the availability of a telephone number, i.e., the inverse of the inclusion probability of an individual.
Results
Testing the sampling design
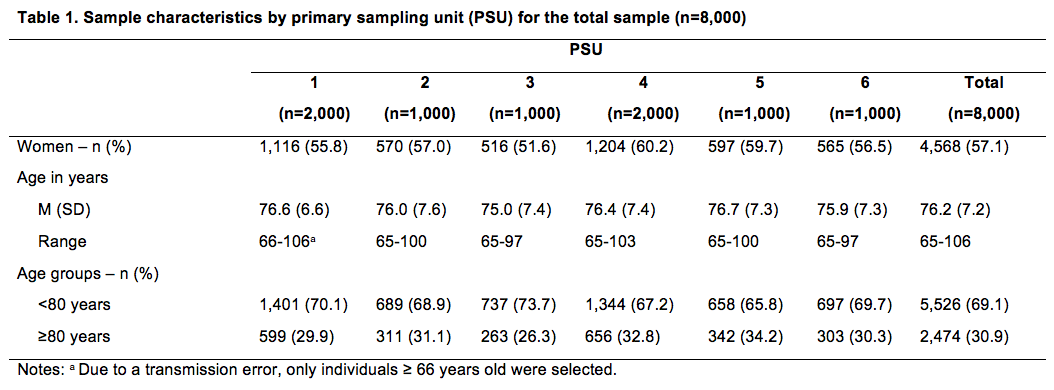
Sample characteristics of the total sample by PSU are depicted in Table 1. Of the total sample, 57.1% were female, and 30.9% were 80 years of age and older. The mean age was 76.2 years (SD=7.2; range: 65-106).
The proportions of nursing home residents identified according to the three different identification strategies are displayed by PSU in Table 2. Handling of the information release ban differed by registration authority. One registration authority excluded individuals assigned with an information release ban before drawing the sample, and two further registration authorities did not send the information ban itself but included individuals with information release bans during the sample drawing. Therefore, the proportions of individuals having an information release ban varied from 0.0% to 6.0% across the PSUs (Table 2). In the total sample, 1.5% of the individuals had an information release ban, and an additional 0.3% of individuals were living at an address where someone else with an information release ban was living but did not have an information release ban in the population register themselves. After restricting the analysis to those PSUs where the registration authorities included individuals having a ban and shared that information, the total percentage of those having an information release ban or living at an address with an associated ban increased to 3.5% (Figure 2).
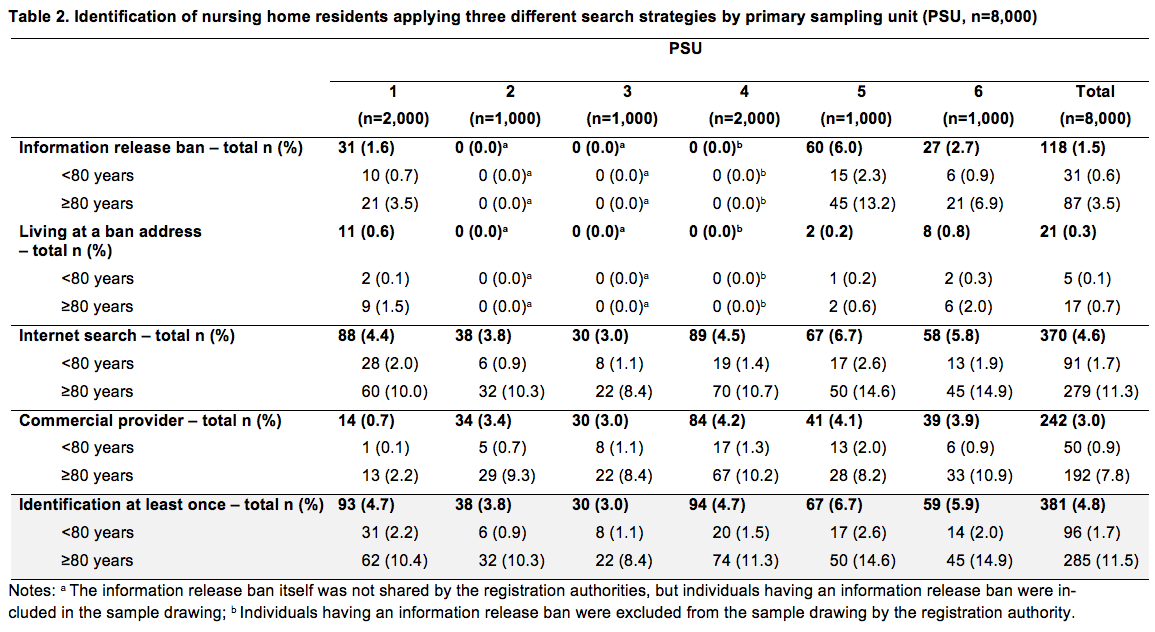
Figure 2. Proportions of nursing home residents according to identification strategy (n=8,000)
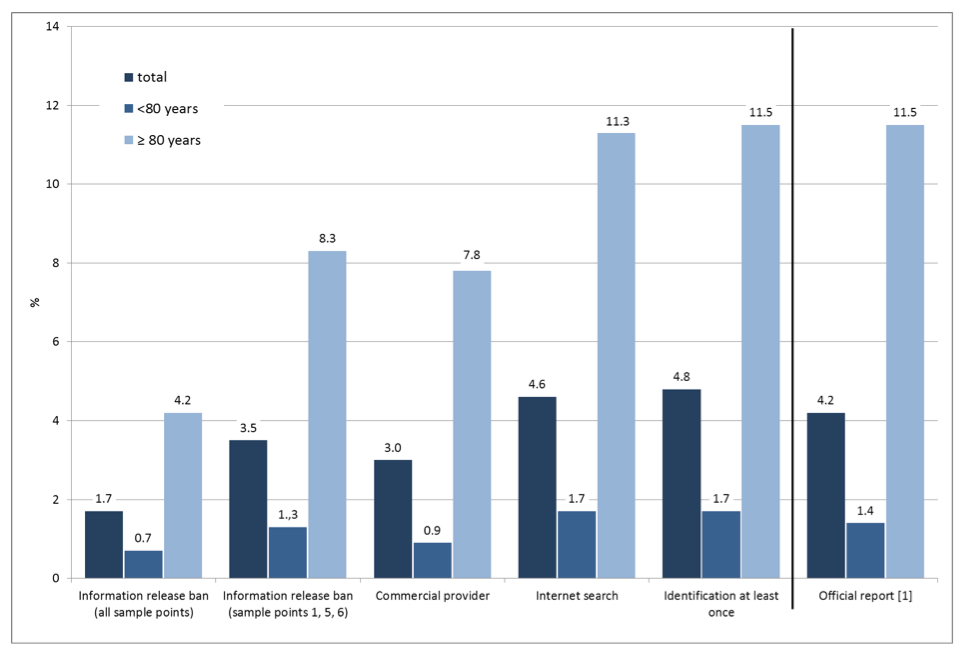
Within the entire sample, the percentages of nursing home residents identified by internet search and by the data provided by a commercial provider were 4.6% and 3.0%, respectively (Table 2). In total, 4.8% of the sample was identified as a nursing home resident by at least one of the three identification strategies (11.5% for individuals 80 years of age and older vs. 1.7% for individuals 65 to 79 years of age). Higher proportions of nursing home residents were found for individuals 80 years of age and older compared to those younger than 80 years of age across all nursing home variables.
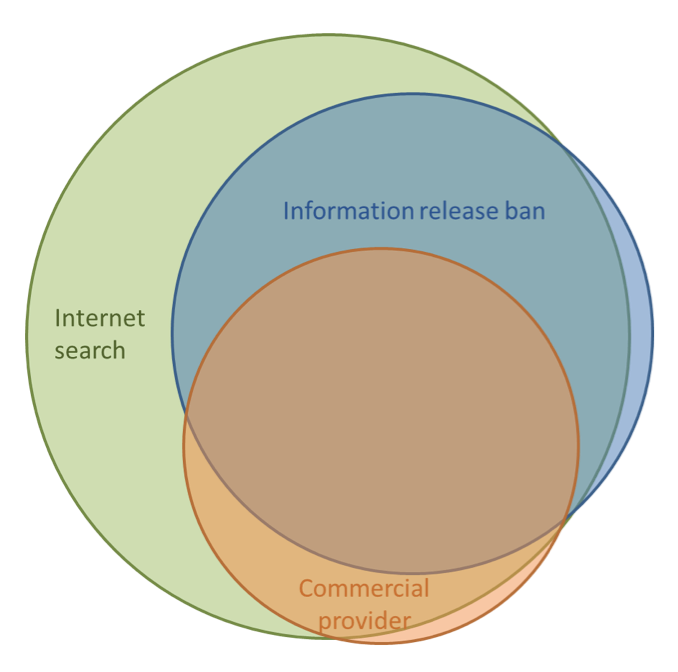
Figure 3 displays the accordance of the three nursing home residents’ identification strategies for PSUs 1, 5 and 6, which shared the information release ban data. Internet searches covered nearly all nursing home residents identified by the two other identification strategies.
Figure 3. Accordance of the three nursing home residents’ identification strategies (only primary sampling units (PSUs) 1, 5 and 6; n=4,000)
Testing of the survey design
Of the total subsample where the survey design was tested (n=2,000), 103 individuals were identified as nursing home residents. Of all nursing home residents, 42.7% lived in the urban, western PSU 1. Compared to those living in private households, nursing home residents were significantly more often female (70.9% vs. 56.3%) and older (≥ 80 years: 70.9% vs. 28.4%), less often married or living in a registered partnership (17.5% vs. 59.6%) and less often of non-German citizenship (1.0% vs. 4.9%).
The sequential mixed-mode design indicated that crude contact rates after the initial postal contact were 25.2% for the nursing home residents and 52.9% for the individuals living in a private household. Telephone contact was not a successful measure for reaching nursing home residents, as a telephone number was available for only three of them, none of whom were randomly selected for telephone recruitment. As a result, all remaining nursing home residents who were randomly selected for further recruitment received a home visit announcement letter and, if applicable, home visit(s) afterwards.
Of all eligible nursing home residents, 20.0% participated in the study compared to 45.9% of the individuals living in a private household (p<0.001; Table 3). Differences were also observed for contact rates, as 49.0% of the nursing home residents but 72.9% of the persons in private households could be contacted (p<0.001). The cooperation rate was also lower among nursing home residents (40.8%) than in persons in private households (63.0%; p=0.002). As these rates did not take into account the random selection of initial non-respondents who received further recruitment efforts, we extrapolated rates for the random selection of subsamples for telephone or personal recruitment. The extrapolated response rates remained lower among nursing home residents than in private household members (31.1% vs. 52.8%), as did the extrapolated cooperation rates (32.8% vs. 56.0%). However, no difference was seen between the extrapolated contact rates of nursing home residents and those living in private households (94.9% vs. 94.3%).
Discussion
One of the objectives of the pilot study IMOA was to assess the coverage of nursing home residents in a register-based random sample in Germany. A substantial proportion of nursing home residents were included in the total register-based sample in the pilot study. Compared to official reports that estimate that 1.4% of individuals 65 to 79 years of age and 11.5% of those 80 years and older are nursing home residents [1], identification of nursing home residents by internet search, including an online database, was found to be the best identification strategy (65-79 years: 1.7%, ≥80 years: 11.3%). In contrast, the proportion of nursing home residents appeared to be underestimated when the other two strategies to identify them were used (information release ban and commercial provider).
This result was especially surprising with regard to the incomplete implementation of the information release ban, as according to the Federal Act on Registration, the ban should be assigned to all institutionalized individuals, including nursing home residents in Germany [11]. However, the Federal Act on Registration was enacted on 01.11.2015. To date, there has been a lack of standards regarding its implementation and the sharing of corresponding addresses, which is also apparent in our results. The inconsistent implementation might even occur within a single registration authority. For example, in the PSU that excluded individuals who had an information release ban before the sample was drawn, the proportion of nursing home residents identified by internet search was still as high as could have been expected by official reports (PSU 4: 4.5%).
Furthermore, our data indicate that among people 65 years and older, an information release ban is applied almost exclusively for nursing home residents, and therefore, this approach almost precisely identifies them. In our sample, there were only four individuals with an information release ban who were not also identified as nursing home residents by internet search. Further evaluation of postal addresses showed that only one of these individuals was not living in a nursing home. If the implementation of information release bans becomes a standard procedure for all municipal authorities, it could function as a standard identification strategy for nursing home residents aged 65 years and older in Germany in the future.
However, the information release ban is not available for all PSUs and thus cannot be utilised as a standard identification strategy for nursing home residents. According to Section 34, sentence one, Number 13 Federal Act on Registration [11], the registration authorities are legally authorized to share this information with other authorities such as the Robert Koch Institute, as it is a Federal Institute within the portfolio of the Federal Ministry of Health. In general, this was not clear to the registration authorities, and some were highly concerned about data protection. These concerns were not allayed after submitting the study approvals from the Federal Commissioner for Data Protection and Freedom of Information and an ethics committee. When in doubt, the registration authorities did not share this critical information and, therefore, acted as gatekeepers. As a result, to date, register-based samples are characterized by an undercoverage of nursing home residents in Germany.
Although the results of internet searches, including online databases, are convincing regarding the identification of nursing home residents, implementation of this personnel-intensive search strategy in a national health monitoring survey with a high number of PSUs does not seem feasible. In addition, this search strategy has some limitations regarding over- and underestimation of the proportion of nursing home residents. First, in German, ‘nursing home’ is not an established term. A variety of other terms exist that cover special living arrangements for older or cognitively/physically impaired individuals. Therefore, it is difficult to generate valid PSU-specific nursing home lists via internet search. For the same reason, a misclassification of nursing home resident status may occur. For example, some individuals might have been incorrectly identified as nursing home residents in our study, as they may have been living in other types of retirement homes without need of care. In addition, nursing home residents could still be registered with their original private home address and would not be identified [20]. Thus, other sampling procedures, such as dual-frame sampling [21, 22], will also have to address similar difficulties. In addition, complete lists of addresses of nursing homes are difficult to obtain in Germany due to the high fluctuation of nursing homes existing lists are often outdated.
The second objective of this study was to test the effect of the sequential mixed-mode design on response, cooperation and contact rates of nursing home residents compared to individuals living in private households. The crude response, contact and cooperation rates of the adjusted gross samples were significantly lower among nursing home residents than in private household members. Regarding response rates, we estimated that 31.1% of nursing home residents and 52.8% of those living in private households would have participated in our study if all initial non-respondents had received further recruitment. Our results indicate that establishing contact by post, and especially by telephone, is not suitable for nursing home residents. The crude contact rate for nursing home residents was only 25.2% after the initial postal contact. Telephone recruitment does not seem feasible, as it was not possible to identify a telephone number for nearly any of the nursing home residents in our sample. Therefore, in population-based health surveys aiming to include nursing home residents, face-to-face contact appears to be the only feasible contact mode if postal contact fails. Our study did not include or evaluate more intensified or more suitable recruitment strategies for nursing home residents, such as involving nursing home management and staff at an early stage of the research project, which could be crucial for the recruitment of nursing home residents [12]. However, we attempted to evaluate whether survey design features that can be implemented in regular health monitoring surveys are sufficient for reaching this target group. Additionally, the study design offered interview assistance, proxy participation and, when necessary, informed written consent by a legally authorized representative. However, these options were rarely used [for more information see 16].
The resources for our pilot study were limited, which led to some limitations for our study design. First, only a limited number of PSUs could be included. Therefore, the data are not representative of all of Germany. Hence, we cannot provide information on how many PSUs provide information release bans in Germany or, even more importantly, how many PSUs systematically exclude persons with implemented information release bans from sampling. However, our selection exhibited some heterogeneity regarding rural/urban and east/west areas, as well as the inclusion of six federal states. Therefore, our findings, especially regarding the handling of the information release ban, show some heterogeneity as well and might be exemplary of Germany. Moreover, our findings can hardly be transferred to other countries as the conditions for sampling from municipal registers differ strongly by country [2].
Second, due to limited resources, we could apply sequential recruitment including home visits to only a random subsample of initial non-respondents. Thus, nearly half of the nursing home residents were initial non-respondents who were not further contacted and resulted as non-contacts. Therefore, the crude response rate for nursing home residents was quite low. However, as the subgroups for further recruitment were randomly selected, we were able to extrapolate our response rates.
To conclude, nursing home residents were included in samples drawn from municipal registration offices in Germany. Nevertheless, such samples are at risk of undercoverage in regards to nursing home residents for whom an information release ban is recorded in the population registers. The response, cooperation and contact rates of nursing home residents clearly lie below the rates of individuals living in private households. Therefore, more time- and cost-intensive survey design features are needed to increase the participation rates of nursing home residents in health studies. To accomplish this, it is critical to identify nursing home residents in the sample before the data collection period starts. However, the identification of nursing home residents in a sample is either insufficient when using easy-to-obtain information such as nursing home address lists by commercial providers or their identification is not possible, as the information release bans are not provided by all registration authorities. It is unlikely that internet searches, while the most effective but most personnel-intensive identification strategy, can be implemented in national health monitoring surveys including hundreds of PSUs. If the implementation of information release bans becomes a standard procedure across all municipality authorities, it could function as a standard identification strategy for nursing home residents in the future.
However, even if this becomes possible, it remains to be seen whether these time- and cost-intensive survey design features needed for nursing home residents can be implemented in regular national health monitoring programmes. Furthermore, even when more effective measures can be implemented, it is doubtful that a sufficiently large subsample of nursing home residents can be reached through general, population-based surveys to calculate reliable health estimates. Therefore, we assume that other methods are needed for nursing home residents. Studies focusing solely on nursing home residents could provide better health report data for them than general population studies, as more intensified and target-group specific recruitment strategies could be incorporated.
References
- Statistisches Bundesamt. Pflegestatistik 2015. Pflege im Rahmen der Pflegeversicherung. Deutschlandergebnisse. . 2017 [cited 2018 12/03]; Available from: https://www.destatis.de/DE/Publikationen/Thematisch/Gesundheit/Pflege/PflegeDeutschlandergebnisse.html.
- Schanze, J.-L., Report on sampling practices for the institutionalized population in social surveys. Deliverable 2.16 of the SERISS project funded under the European Union’s Horizon 2020 research and innovation programme GA No: 654221. 2017.
- Kamtsiuris, P., et al., [The first wave of the German Health Interview and Examination Survey for Adults (DEGS1): sample design, response, weighting and representativeness]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz, 2013. 56(5-6): p. 620-30.
- Klaus, D., et al., Cohort Profile: The German Ageing Survey (DEAS). Int J Epidemiol, 2017. 46(4): p. 1105-1105g.
- World Medical Association. WMA Declaration of Helsinki – Ethical Principles for Medical Research Involving Human Subjects. 2013 [cited 2018 13.11]; Available from: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/.
- Feskens, R.C.W., Difficult Groups in Survey Research and the Development of Tailor-made Approach Strategies. 2009, Utrecht University.
- Kelfve, S., M. Thorslund, and C. Lennartsson, Sampling and non-response bias on health-outcomes in surveys of the oldest old. Eur J Ageing, 2013. 10(3): p. 237-245.
- Kelfve, S., Underestimated Health Inequalities Among Older People-A Consequence of Excluding the Most Disabled and Disadvantaged. J Gerontol B Psychol Sci Soc Sci, 2017.
- Keyes, K.M., et al., How Healthy Are Survey Respondents Compared with the General Population?: Using Survey-linked Death Records to Compare Mortality Outcomes. Epidemiology, 2018. 29(2): p. 299-307.
- Riedel-Heller, S.G., A. Busse, and M.C. Angermeyer, Are cognitively impaired individuals adequately represented in community surveys? Recruitment challenges and strategies to facilitate participation in community surveys of older adults. A review. Eur J Epidemiol, 2000. 16(9): p. 827-35.
- Federal Ministry of the Interior. Federal Act on Registration of 3 May 2013 (Federal Law Gazette I p. 1084), as last amended by Article 11 of the Act of 18 July 2017 (Federal Law Gazette I p. 2745). 2017 18.07. [cited 2018 14.05.]; Available from: https://www.gesetze-im-internet.de/englisch_bmg/englisch_bmg.html.
- Mody, L., et al., Recruitment and retention of older adults in aging research. J Am Geriatr Soc, 2008. 56(12): p. 2340-8.
- Hall, S., S. Longhurst, and I.J. Higginson, Challenges to conducting research with older people living in nursing homes. BMC Geriatr, 2009. 9: p. 38.
- Jacelon, C.S., Older adults’ participation in research. Nurse Res, 2007. 14(4): p. 64-73.
- Wagner, M., et al., Quality of life of the very old : Survey on quality of life and subjective well-being of the very old in North Rhine-Westphalia (NRW80+). Z Gerontol Geriatr, 2018. 51(2): p. 193-199.
- Gaertner, B., et al., Effects of a sequential mixed-mode design on participation, contact and sample composition – Result of the pilot study „IMOA – Improving Health Monitoring in Old Age“ submitted.
- Wohnen im Alter Internet GmbH. Wohnen im Alter – Das Onlineportal für Wohnen & Pflege. 2017 [cited 2018 14.05.]; Available from: https://www.wohnen-im-alter.de/einrichtung/pflegeheim/deutschland.
- The American Association for Public Opinion Research (AAPOR), Standard Definitions: Final Dispositions of Case Codes and Outcome Rates for Surveys. 2016.
- StataCorp., Stata Statistical Software: Release 15. 2018, StataCorp LLC: College Station, TX.
- Diederichs, C., R. Pohlmann, and K. Berger, [The frequency of older people living in nursing homes: results from a population-based study in Dortmund]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz, 2010. 53(5): p. 504-9.
- McHenry, J.C., et al., Recruitment of Older Adults: Success May Be in the Details. Gerontologist, 2015. 55(5): p. 845-53.
- Metclaf P and S. A., Using multiple frames in health surveys. Stat Med. , 2009. 55(5): p. 845-53.23.
- The American Association for Public Opinion Research, Survey Outcome Rate Calculator 4.0. 2016.
-
Keywords
calibration CATI coverage coverage bias cross-national surveys data linkage data quality European Social Survey experiment face-to-face face-to-face survey Facebook hard to reach populations incentives item nonresponse measurement measurement error mixed-mode surveys multitasking non-probability samples Nonresponse nonresponse bias nonresponse rates paradata PIAAC Probability sample probability samples QR codes rare populations response rate Satisficing social desirability Social media survey survey-taking climate survey data survey management survey methods Telephone survey telephone surveys total survey error unit nonresponse validity web survey Web surveys weighting
