

From peer to peer: Reaching migrants from sub-Saharan Africa with research on sexual health utilizing community-based participatory health research
Koschollek C., Kuehne A., Amoah S., Batemona-Abeke H., Bursi T.D., Mayamba P., et al. (2019). From peer to peer: Reaching migrants from sub-Saharan Africa with research on sexual health utilizing community-based participatory health research. Survey Methods: Insights from the Field. Retrieved from https://surveyinsights.org/?p=10812
© the authors 2019. This work is licensed under a Creative Commons Attribution 4.0 International License (CC BY 4.0) 
Abstract
Migrants from sub-Saharan Africa (misSA) in Germany are disproportionally affected by HIV. To develop targeted interventions, it is necessary to collect data on knowledge, attitudes, behaviour and practices (KABP) regarding HIV and sexual health. However, misSA are difficult to reach and to sample: a) it is unknown how many people with an African migration background are living in Germany, and b) HIV and sexual health topics are highly stigmatized in these communities. We utilized a community-based participatory health research approach to develop a study protocol and conducted a KABP survey on HIV and sexual health among misSA in six German cities between 2015 and 2016. A convenience sample of 2,879 participants was recruited by 99 trained peer researchers through outreach in their local communities. Due to steering of recruitment, the study population reflected the official registered misSA population well and was diverse in terms of sociodemographic characteristics. Peer researchers mainly recruited participants that were similar to themselves with regard to gender, age and regions of origin. Male and younger peer researchers more often recruited participants from vulnerable sub-groups like migrants with a probably undocumented legal status who could not have been reached by probability sampling based on population registers.
Keywords
community-based participatory health research, HIV, KABP survey, migrants from sub-Saharan Africa, peer research, survey methods
Acknowledgement
The authors would like to thank all study participants, who took the time to answer all these questions, and our local partner organizations as well as the colleagues at the local public health departments who supported our study. We also want to thank the expert group who advised study planning and conduction: Robert Akpabli, Alphonsine Bakambamba, Johann Fontaine, Tanja Gangarova, Line Göttke, Silke Gräser, Holger Hanck, Hans Hengelein, Silke Klumb, Gesa Kupfer, Elizabeth Lolo, Clement Matweta, Pierre Mayamba, Brigitte Menze, Heidrun Nitschke, Hapsatou Oudini, Omer Idrissa Ouedraogo, Gerhard Peters, Katja Römer, Antje Sanogo, Ute Schwartz, Nozomi Spennemann, Ursula von Rüden, Hella von Unger, Mara Wiebe, and Michael Wright. And last but not least we warmly want to thank the peer researchers without whom this project could not have been realized.
Copyright
© the authors 2019. This work is licensed under a Creative Commons Attribution 4.0 International License (CC BY 4.0)
Background
HIV in migrants from sub-Saharan Africa living in Germany
Migrants from sub-Saharan Africa (misSA) in Germany are disproportionally affected by HIV. In 2016, 3,419 new HIV diagnoses were reported to the Robert Koch Institute (RKI), the majority of these notifications included information on country of origin of the respective person (3,235). Among these 14.9% of diagnoses were among misSA (n=483) [1]. Surveillance and study data suggest a high vulnerability of misSA for late presentation to diagnosis and care [2-4] due to a lack of access to HIV counselling, testing and health care in general. This might especially be the case for misSA with an undocumented legal status, due to legal regulations and possibly existing knowledge gaps regarding the German health care system [5-8].
Migrants from sub-Saharan Africa in HIV research
The European Centre for Disease Prevention and Control recommends behavioural surveillance on knowledge, attitude, behaviour and practice (KABP) regarding HIV and other sexually transmitted infections (STI) among the general population as well as among migrant and ethnic minority populations who are most affected by HIV [9]; in Germany this is the case for misSA. However, this group is not sufficiently reached by HIV/STI surveys addressing the general population [10].
One reason for that is that misSA are just a small group within the population in Germany. At the end of 2016, 339,205 people with a sub-Saharan African citizenship were registered at the German foreigners’ registration offices (foreigners’ statistics) [11] which equals 0.4% of the German population [12]. In addition to those misSA registered at the foreigners’ registration offices, an unknown number of people with a sub-Saharan African migration background have a German citizenship, as well as an unknown number of African people with an undocumented legal status contribute to the unknown number of misSA in Germany. All three groups, registered foreigners, misSA with German citizenship and undocumented migrants are part of the target population. Thus, it is not possible to draw a random sample, as it is unclear how many people with a sub-Saharan African migration background are living in Germany. Drawing a sample from residents with a sub-Saharan African citizenship on basis of population registers is an option, but doing so would miss those with German citizenship as well as those with an undocumented legal status which are a particular vulnerable group for HIV transmission.
HIV is a highly stigmatized topic in sub-Saharan African countries [13, 14] but also within African communities living outside of the African continent [15-17]. This affects the willingness to be interviewed, as sensitive topics like sexual behaviour might lead to inaccurate answers or a high item nonresponse [9, 18]. To overcome this, a profound explanation of the study’s aims to potential participants is essential and also trust is crucial in approaching people with such a topic.
One possibility to deal with these issues is to utilize approaches of community-based participatory health research (CBPHR), which are especially feasible to reach vulnerable sub-populations like recent migrants or those with an undocumented legal status [19, 20]. CBPHR approaches were shown to be feasible and successful in larger international [21, 22] as well as in smaller, local surveys in Germany addressing misSA with the topic of sexual health and HIV [23-26]. CBPHR aims at involving members of the group under study throughout the whole research process: study planning, data collection and interpretation of results as well as the formulation of recommendations [19, 27-29]. To involve the group under study within the process of data collection, one option is to work with peer researchers, who are active members of the group under study with well-established networks and who recruit study participants within their communities. This method of data collection proved to be feasible and successful in studies with misSA internationally as well as in Germany [21-23, 25, 30, 31]. Although such convenience sampling approaches cannot be representative for the whole population under study, they proved to be the only promising way to overcome sampling and recruitment barriers, when a sampling frame is missing and the topic under study is highly sensitive. Therefore, we decided to work with peer researchers to collect data on KABP in misSA residing in Germany when conducting the study on sexual health among migrants from sub-Saharan Africa in Germany (misSA study).
Objectives
Within this paper we will focus on the process of data collection and describe the effects of working together with peer researchers on the sample composition and reachability of particular hard-to-be-reached sub-groups among the target population. The overarching aim of this paper is to inform future research on how particular sub-groups of misSA can be better reached by different efforts while utilizing methods of CBPHR. We therefore, a) describe who reaches whom in terms of sociodemographic characteristics of peer researchers and participants and b) describe the process of steering of recruitment to reach particular hard-to-be-reached sub-groups within the target population. We furthermore c) analyse the association between mode of questionnaire administration and the participation of different sub-groups.
Methods
Study design
We conducted a cross-sectional survey on KABP regarding HIV and sexual health among misSA between 2015 and 2016 in the cities and regions of Munich, Rhine-Ruhr region, Cologne, Berlin, Frankfurt am Main and the region Hannover. Cities and regions were chosen according to the number of people with a sub-Saharan African citizenship being officially registered according to foreigners’ statistics and to the availability of a potential partner organization there. For every study city we did an analysis of the local communities beforehand using data from the foreigners’ statistics on area level from 2013[1] [32]. These data enabled us to describe at least a part of the local misSA communities in terms of gender and citizenship, excluding misSA with German citizenship and those with an undocumented legal status. Information on other sociodemographic characteristics regarding the composition of the local communities was not available.
In each study city we collaborated with a partner organization that had established contacts to the local African communities and recruited a local study coordinator and peer researchers. Peer researchers were active members of the local African communities with extended networks and interest in the topic of HIV. Furthermore, they had to be at least 18 years of age. They were recruited from the prevailing African communities in the respective city or region identified within the analysis of foreigners’ statistics as we aimed to have the local communities represented in the group of peer researchers, at least in terms of characteristics we knew from a part of the target population, i.e. gender and citizenship. The peer researchers had various backgrounds with regard to school education, time living in Germany, languages spoken and religious affiliation. Peer researchers received a two-day training involving the respective partner organization, RKI and peer researchers from former study cities covering the topics of a) study design and questionnaire contents, b) research ethics and informed consent, c) recruitment strategies and d) information on HIV and STI. Training on recruitment strategies included a community mapping to identify relevant places for recruitment, e.g. churches, mosques, afro shops, meeting places or train stations. After the training, peer researchers started recruitment of study participants through outreach in their local communities and at places identified during the community mapping. The number of participants to be recruited was determined by the size of the local misSA population being officially registered in the respective city or region [33].
Data collection
Ten to 25 peer researchers per study city recruited participants during ten to twelve weeks. The number of peer researchers was dependent on the number of participants to be recruited as well as on the resources of the partner organization, i.e. how many peer researchers they were able to recruit or how many peer researchers they were able to supervise during the process of data collection. Peer researchers received a payment of 20 euros per recruited participant if at least 60% of the questions were answered, including information on gender and own and parents’ sub-Saharan African countries of birth. The decision to compensate them on basis of submitted questionnaires instead of worked hours was based on a better calculability beforehand as well as administrative preferences by partner organizations. Peer researchers in the first study city were paid for a maximum of 50 questionnaires; in the following study cities this cut-off point was set at 20 to 30 questionnaires. In addition, peer researchers were paid for taking part in the training, evaluation meetings and focus group discussions which were arranged for interpretation of results and formulation of recommendations.
Participation in the study was possible by filling in a paper-based standardized questionnaire or by participating in a personal or telephone interview with a peer researcher. Peer researchers marked their questionnaires with a unique identifier before handing them out or conducting the interview and noted the mode of administration; together with the questionnaire language this information is defined as administrative information in the following. Questionnaires were sent back to RKI by participants or peer researchers in post-paid envelopes. Upon arrival of the questionnaire, we entered administrative information as well as sociodemographic characteristics of participants. The local study coordinator and peer researchers received weekly feedback from RKI on the following administrative information i) number of questionnaires per peer researcher, ii) modes of administration and iii) languages of questionnaires. They also received weekly feedback on sociodemographic characteristics of participants in terms of i) gender, ii) age, iii) country of birth, iv) time living in Germany, v) level of education, vi) religious affiliation and vii) health insurance status. We used this information to steer recruitment. Data on gender and countries of birth were compared to official data from foreigners’ statistics, where gender and citizenship are registered of at least a part of the target population. Peer researchers were then encouraged to recruit underrepresented groups, e.g. misSA originating from certain countries. In addition, we used peer researchers’ information on the composition of their communities in terms of other sociodemographic characteristics to steer recruitment as they were experts of their own living situation and knew best how their communities are comprised. After four weeks of data collection, a meeting for process evaluation was conducted with peer researchers, local study coordinator and RKI to evaluate how recruitment worked, to discuss recruitment strategies as well as which groups might be underrepresented and how accessibility to these groups might be improved; e.g. to recruit more people with higher educational levels e.g. at universities or to recruit more women e.g. in times when they might fetch their children from kindergartens. More details on study planning, the pilot study in Hamburg, the study design including sample size calculations as well as first results of the main study are published elsewhere [31, 33-36].
Ethics statement
No names or addresses of participants were recorded and verbal consent to take part in the survey was obtained by peer researches before handing out the questionnaire or doing an interview. The Commissioner for Data Protection of the RKI approved the study in January 2015, full ethical clearance has been granted by the Ethical Committee at the medical school of Charité, Berlin in November 2014 (EA4/105/14). The study was funded by the German Federal Ministry of Health.
Data analyses
Local study coordinators collected the following sociodemographic information from peer researchers i) gender, ii) age and iii) country of birth or countries of birth of parents if peer researchers were born in Germany. Countries of birth were grouped as regions according to the Federal Statistical Office [11, 37].
For our analyses, we excluded questionnaires from participants recruited by local study coordinators, because their role in the study differed from the peer researchers’. We also excluded cases where the unique identifier of the peer researcher was missing.
Sociodemographic characteristics of peer researchers as well as those of participants were tabulated and stratified by study cities. To detect differences in characteristics of peer researchers between study cities we used Fisher’s exact test due to the small numbers (Table 1). To detect differences in recruitment strategies (administrative information, Table 1) and the study population (Table 2) between study cities we used chi-squared tests, excluding categories “ambiguous”, “unknown” as well as “Europe, other countries, unknown” if numbers were too small and therefor only reporting numbers and no proportions in these categories. Peer researchers and recruited participants were matched by the unique identifier of each peer researcher. To describe who reached whom, we stratified sociodemographic characteristics of the participants by gender and age of the peer researchers, which was dichotomized at the median age of peer researchers, and conducted univariable logistic regression analyses and calculated unadjusted odds ratios (OR) and 95% confidence intervals (CI) to evaluate if characteristics of peer researchers had an impact on the accessibility of certain sub-groups among participants. To determine if peer researchers utilized different recruitment strategies, administrative information (mode of administration, language of questionnaire) was analysed similarly.
Furthermore, differences in mode of administration between sub-groups of participants were analysed using univariable logistic regression analyses; unadjusted OR and 95% CI were calculated. Personal and telephone interviews were summed up to dichotomize the mode of administration, as numbers of telephone interviews alone resulted in very small numbers in stratified sub-group analyses. Differences in medians (age, length of stay in Germany) were analysed using Mann-Whitney-U tests.
Reference categories for univariable logistic regression analyses were either set by taking the midst category of ordinal scaled variables (education, German language skills), the category including the median of ordinal summed up metric variables (age) or the modal category was taken (gender, length of stay in Germany, religious affiliation, health insurance status and region of birth). Setting of reference categories was also led by theoretical considerations, e.g. access to health care (health insurance status).
To analyse how steering of recruitment had worked, we compared proportions of exemplary sub-groups of participants within three of six study cities during the process of recruitment. We compared proportions four weeks before the end of recruitment with correspondent proportions after the end of the recruitment period. For gender distribution and most common citizenships within the respective study city we used data from foreigners’ statistics 2013 [32] for comparison with our samples. Although within the foreigners’ statistics only a sub-group of the target population is registered, we decided for that comparison as we had no other information available on the composition of the local communities regarding gender and countries of birth. In terms of other sociodemographic characteristics we tried to recruit a heterogeneous sample.
Results
In total, we received questionnaires from 3,178 participants, of which 3,040 fulfilled inclusion criteria; overall 48 questionnaires were excluded due to lack of completeness. We are not able to report response rates, as peer researchers did not record how many people they approached. Due to this non-recording of the participation rate the mechanism that is responsible for this surely occurred behaviour can only be modelled as being completely random. For the following analyses we excluded 128 questionnaires of participants who were recruited by four of six study coordinators and 33 questionnaires lacking information on the recruiting peer researcher. This resulted in a final sample size of 2,879 participants recruited by 99 peer researchers.
Characteristics of peer researchers
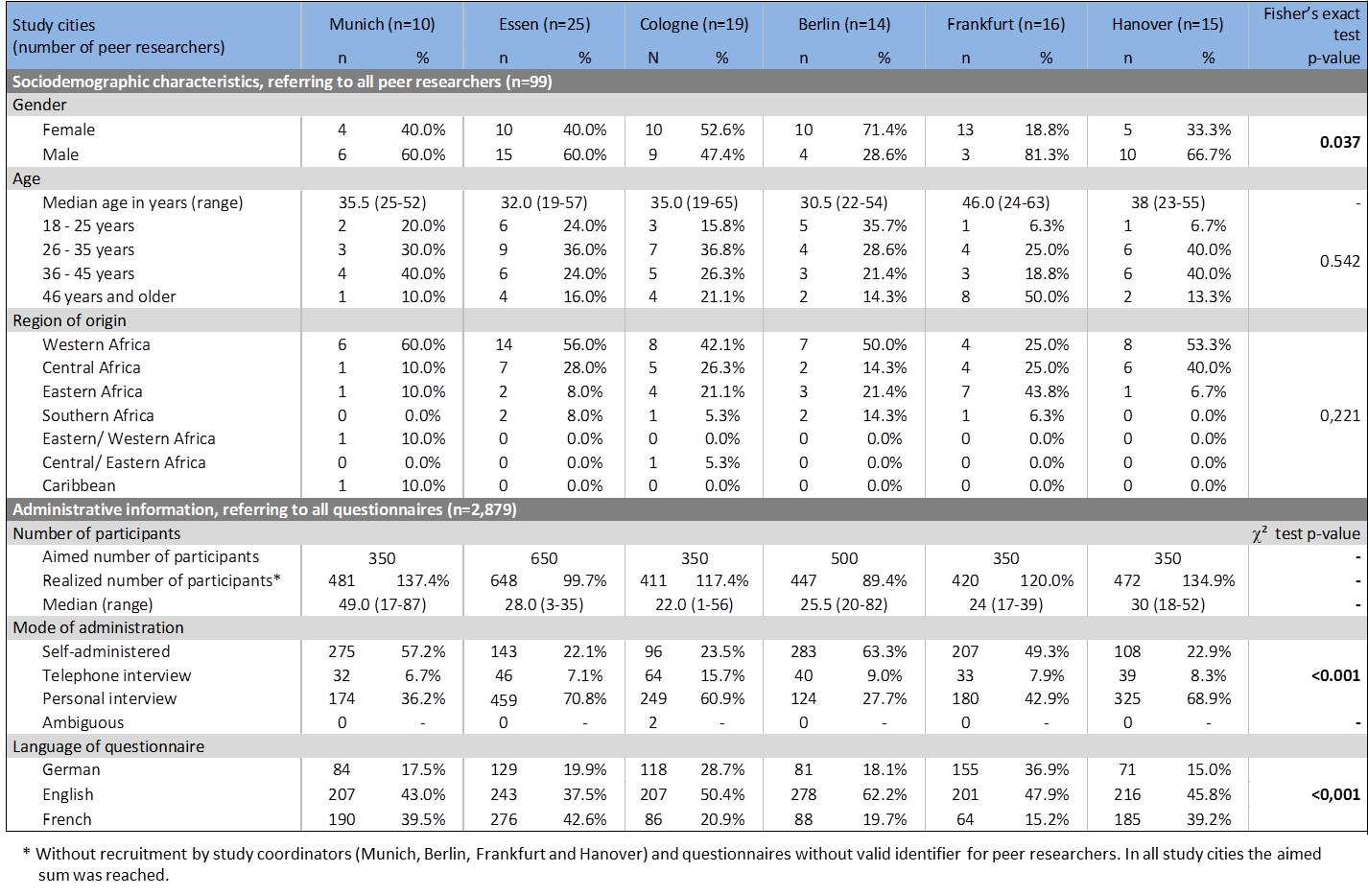
Of 99 peer researchers 52 were female (52.5%), the median age was 35 years, ranging from 19 years to 65 years of age. Peer researchers were born in 22 different sub-Saharan African countries, three were born in Germany and one peer researcher originated from the Caribbean, but had well-established connections to the local African community. Main countries of birth of peer researchers were Nigeria (12.1%), Ghana (12.1%) and Cameroon (11.1%). There were significant differences in terms of gender distribution of peer researchers by study cities, but they did not differ in terms of age and regions of origin (Table 1). While in Berlin and Munich the majority of questionnaires were filled in by participants themselves, in Essen, Hanover and Cologne the majority of participants took part in personal interviews. The questionnaire language differed between the study cities (Table 1).
Table 1: Characteristics of peer researchers (n=99) and administrative information (n=2,879) stratified by study cities, Fisher’s exact and chi² test
Characteristics of the study sample
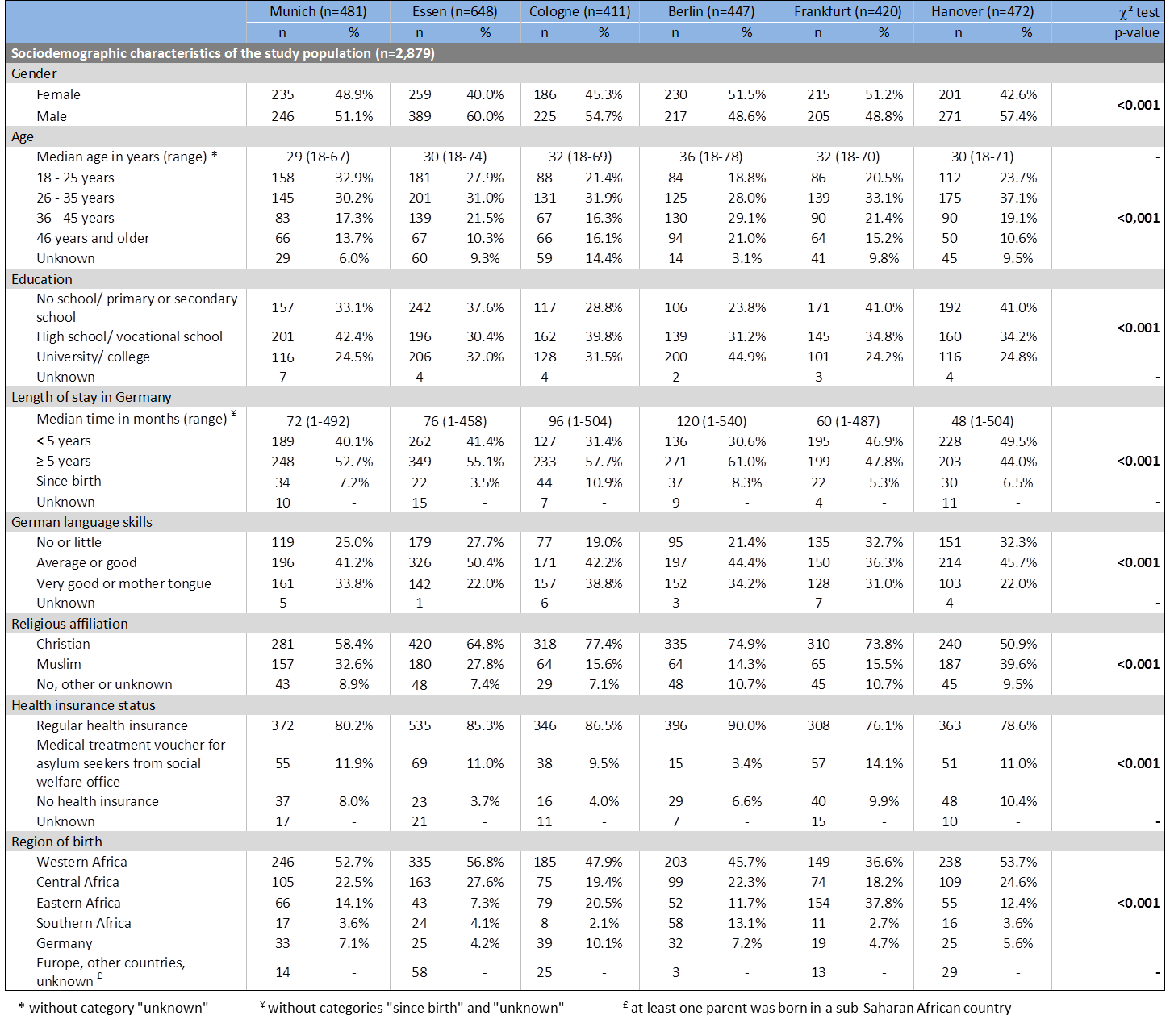
Of 2,879 participants 46.1% were female (n=1,326). The median age was 31 years and age ranged from 18 to 78 years. Two thirds reported to have high school/ vocational school (34.8%) or a university degree (30.1%). Median time living in Germany was six years, ranging from one month to 45 years; 6.6% of the study population reported to live in Germany since birth. Almost half of the participants reported average or good German language skills (43.6%). Two in three participants reported Christian (66.1%) and 24.9% Muslim religious affiliation. Most participants had regular health insurance (80.6%), every tenth was dependant on treatment vouchers from the social welfare office (9.9%) and 6.7% reported to have no health insurance at all. Participants in the study cities differed significantly in terms of gender and age distribution, educational levels, their length of stay in Germany as well as their German language skills, with regards to their religious affiliation, health insurance status and region of birth (Table 2). Overall, participants were born in 52 different countries; main countries of birth were Nigeria, (12.2%), Ghana (11.0%), Cameroon (10.7%), Germany (6.0%) and Togo (5.4%).
Table 2: Sociodemographic characteristics of the study population stratified by study cities, chi² test, n=2,879
Who reached whom?
Of 2,879 participants 51.1% were recruited by female peer researchers (n=1,470) and 52.6% were recruited by peer researchers up to the age of 35 years (n=1,514). Each peer researcher recruited 26 participants in median, ranging from one participant to 87 participants.
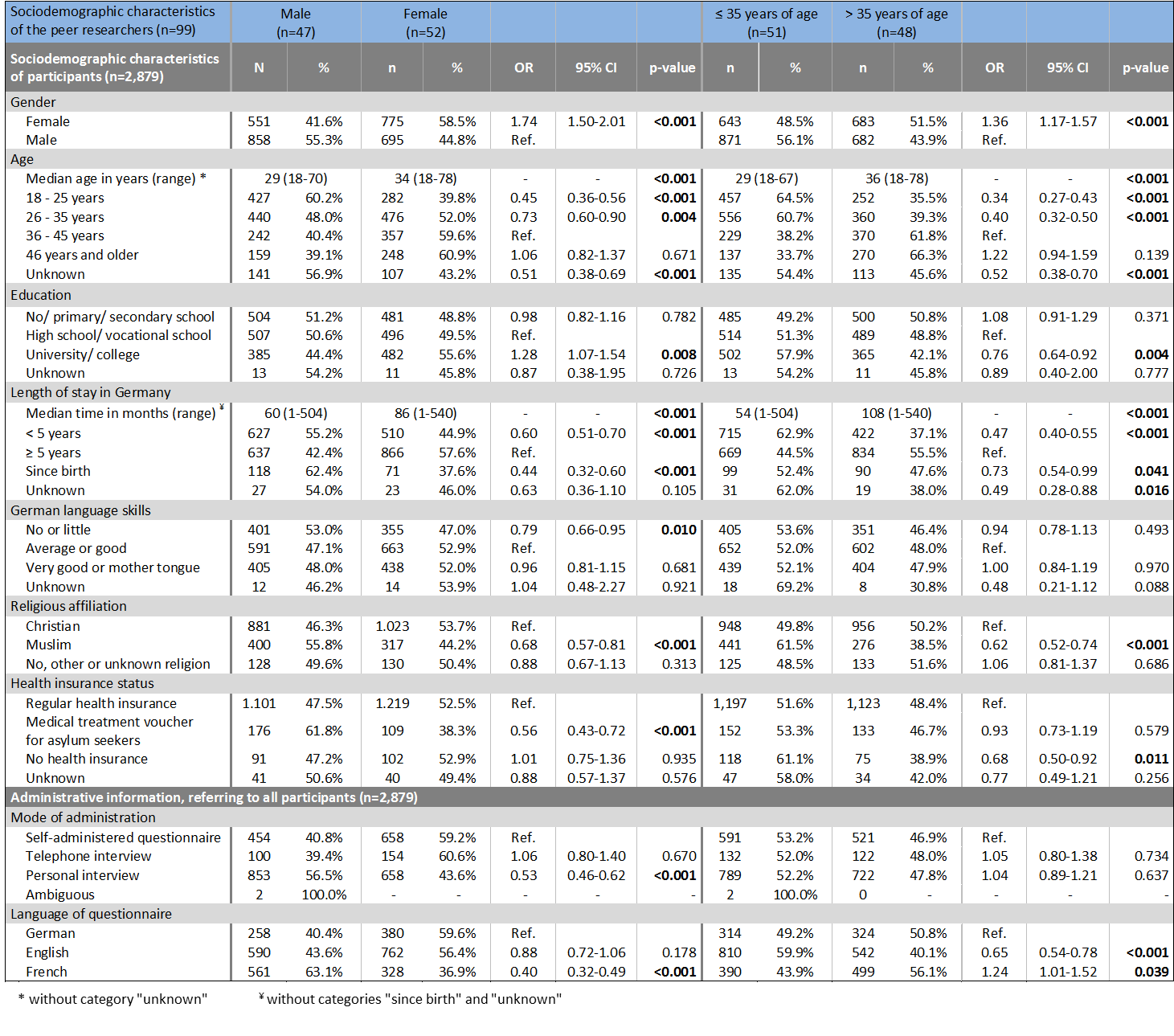
The median age of participants recruited by female peer researchers was higher and the median stay in Germany was longer. Younger participants, people with shorter duration of stay in Germany, those who lived here since birth and participants with Muslim religious affiliation were less often recruited by female peer researchers. In addition, participants with no or little German language skills and those who needed a medical treatment voucher from the social welfare office were less often reached by female peer researchers. However, participants with university or college degree were more often recruited by female peer researchers. Telephone interviews were less often used as a mode of administration by female peer researchers as well as questionnaires in French language (Table 3).
In median participants recruited by peer researchers older than 35 years were older and reported a longer time of stay in Germany than those recruited by younger peer researchers (i.e. ≤ 35 years). Female participants more often were convinced to take part by older peer researchers; younger participants were less well reached by peer researchers older than 35 years as well as those with university or college degree, who lived in Germany for less than five years or since birth, participants with Muslim religious affiliation and those without any health insurance. The different modes of administration were equally used by younger and older peer researchers; French questionnaires were more often and English ones less often used by older peer researchers (Table 3).
Table 3: Comparison of sociodemographic characteristics of the peer researchers to those of participants, univariable logistic regression analysis, n=2,879
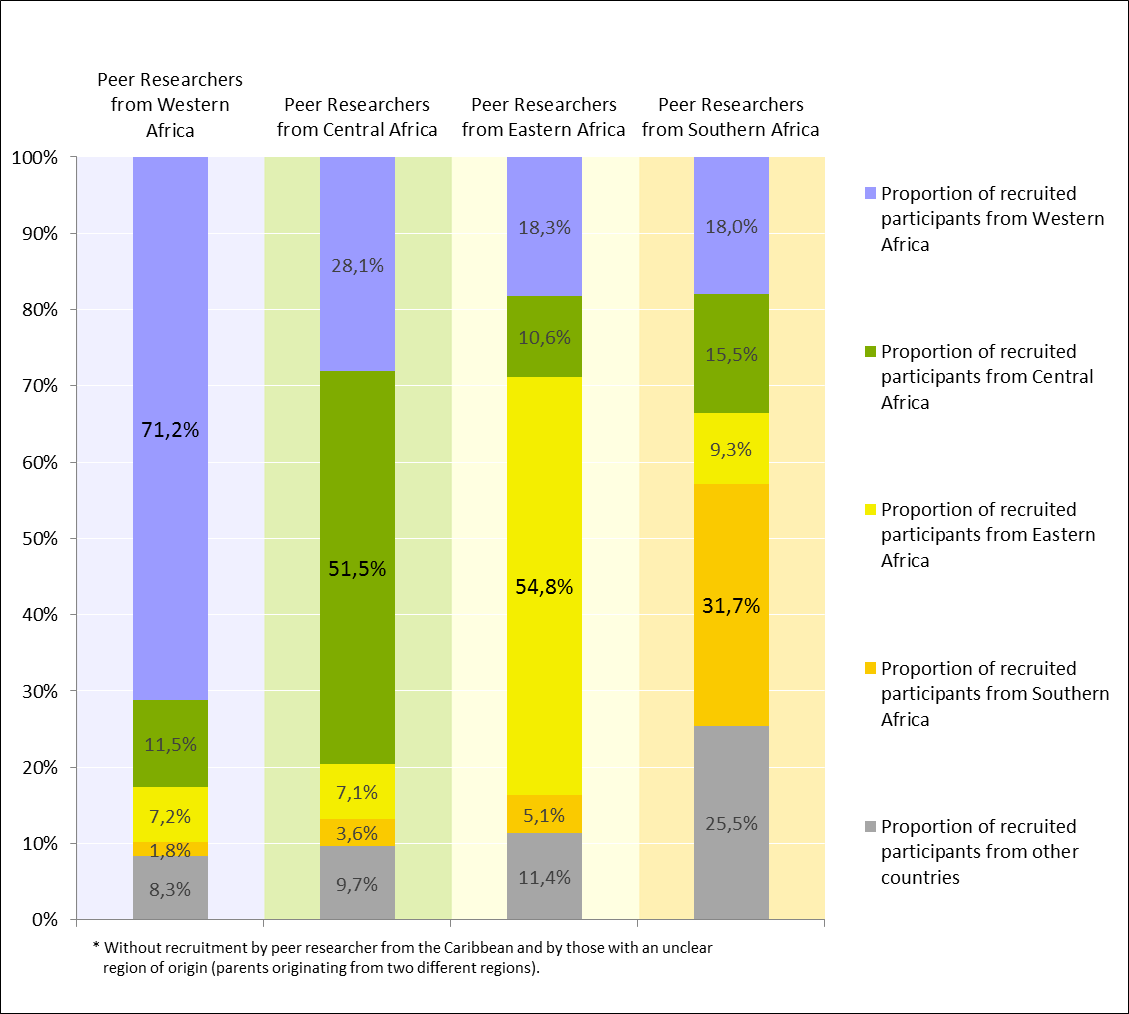
Peer researchers recruited primarily among people originating from the same region or even country as themselves. Half of participants from Ghana (52.5%) were recruited by peer researchers originating from Ghana, and peer researchers from Kenya, Nigeria and Cameroon accounted for nearly half of participants from these respective countries (45.6%, 42.2% and 40.1%).
The majority of participants recruited by peer researchers from Western Africa was born in a country of Western Africa themselves (71.2%) and more than half of participants recruited from peer researchers from Central or Eastern Africa were born in the same region (51.5% and 54.8% respectively) (Figure 1).
Figure 1: Region of origin of peer researchers vs. region of birth of participants, n=2,755*
Mode of questionnaire administration
Choosing to do an interview was negatively associated with female gender, a non-Christian or non-Muslim, an unknown or no religious affiliation, with an unknown health insurance status and with being born in a Southern African country. On the other hand participants with Muslim religion and those being born in Europe, another foreign country or with unknown country of birth more often chose to do an interview (Table 4).
Table 4: Mode of questionnaire administration among sub-groups of participants, univariable logistic regression analysis, n=2,877*

Steering of recruitment
Within the first study city, Munich, underrepresented groups were females, people from Togo and Somalia and participants with Muslim religious affiliation. According to foreigners’ statistics the proportion of females among all registered misSA in Munich metropolitan area at the end of 2013 was 47%. Four weeks before finishing recruitment, the proportion of women within the sample was 42%; peer researchers then tried to recruit more women and finally realised a proportion of 49% women. According to foreigners’ statistics, citizens from Togo were the second most common registered sub-Saharan African group in Munich metropolitan area, whereas Togo ranked 10 in the list of most common countries of birth in the sample. After encouraging peer researchers to increasingly recruit participants from Togolese origin, Togo became the second most common country of birth within the sample. The proportion of Muslim participants, for which we had no official statistics, rose from 28% to 33% within these four weeks.
In Cologne, underrepresented groups were also females (41% vs. 49% according to foreigners’ statistics), participants from Cameroon (seventh most common country of birth in the sample vs. fourth most common citizenship in foreigners’ statistics) and Muslim participants (12%). After steering recruitment, peer researchers were able to increase the proportion of women (45%) as well as of Muslim participants (16%). After adjusting recruitment, people from Cameroon made the fifth most common country of birth in the sample.
Two only small sub-groups in Frankfurt were participants being born in Germany and those without any health insurance. Proportions of both groups could be increased until the end of recruitment. The final proportion of participants being born in Germany rose from 2% to 5% and from participants without health insurance from 7% to 10% in the final sample in Frankfurt.
Discussion
Working together with specifically selected peer researchers as a method of CBPHR allowed us to recruit a heterogeneous sample of misSA living in six German cities. With regards to gender and country of birth our sample reflects the officially registered misSA population in Germany well. The gender ratio in 2013 was 46% females to 54% males [32]; within our final sample we included 46% females as well. The three most common African citizenships in Germany were Ghanaian, Nigerian and Cameroonian [32]; citizenships of these three countries accounted for 36% of all misSA registered at the foreigners’ registration offices in 2013. Nigeria, Ghana and Cameroon were the three most often stated countries of birth within the misSA study, and within the final sample these three countries of birth accounted for 35% of participants.
With regards to all other unknown sociodemographic characteristics we tried to recruit as heterogeneous a sample as possible and our aim was to sufficiently include especially vulnerable sub-groups. With regards to education, we were able to reach more people with lower educational levels than in other European studies targeting misSA [22, 38]. Therefore, we might have reduced educational bias in our survey. We also reached many recent migrants: 25% of misSA within our sample were living in Germany for less than two years and 15% for less than one year. Every sixth participant reported to have no health insurance at all, which was used as a proxy for an undocumented legal status, or to need a medical treatment voucher from the social welfare office which is the case for asylum seekers. Reaching these vulnerable groups of recent and also undocumented migrants was only possible due to the efforts of peer researchers who went to accommodations for asylum seekers or protest camps of refugees [39, 40], to hand out questionnaires or to do interviews. Reaching these groups is of outmost importance for future prevention planning as their access to the regular health care system is limited due to legal regulations but also because of probably existing knowledge gaps about the German health care system. Using methods of probability sampling based on population registers would not have allowed us to reach these sub-groups. People with an undocumented legal status would be missed when drawing a register-based sample. Recent migrants, especially in the first time after their arrival, often live in accommodations for asylum seekers. According to § 52 Federal Act on Registration, addresses of people living in institutions are excluded when drawing register-based samples. In addition, this group is quite mobile, moving from initial reception accommodations to regular accommodations for asylum seekers and finally into permanent housing, which makes addresses often to be out of date resulting in people falling out of the sampling frame.
With regards to who reached whom we can recommend recruiting peer researchers similar to those groups researchers wish to reach, as they mainly recruited people being similar to themselves. Male as well as younger peer researchers were able to recruit more people from vulnerable sub-groups like recent migrants or those without a regular health insurance, which should also be taken into account when recruiting peer researchers. However, steering of recruitment also allowed us to reach all those sub-groups we wanted to reach. To do so, time is the most important prerequisite one needs to have, as this process needed a lot of communication between study coordinators, peer researchers and researchers from RKI. With regards to the mode of administration we found no clear preferences among sub-groups of participants. However, multiple modes of survey administration but above all addressing potential participants personal seem crucial to persuade people to take part in a survey like ours.
As a limitation, we should have collected more information on sociodemographic characteristics from peer researchers, like educational levels, time living in Germany or religious affiliation to deepen the analyses at hand. Furthermore we cannot determine representativeness due to a) the sampling procedure itself and b) the missing sampling frame. Nevertheless, we adjusted recruitment to the only information we had from misSA registered at the foreigners’ registration offices, namely gender and citizenship, assuming that these characteristics of the non-registered population are equally distributed as those within the registered part. Additionally, peer researchers were compensated on basis of submitted questionnaires, which might have induced them to minimise their radius for recruitment or to motivate participants to hastily fill out the questionnaire. We tried to overcome these issues with good training including a community mapping and a lot of information on the background of the study.
However, random sampling and representativeness are challenges researchers generally face when sampling immigrant minorities in Germany, regardless of their origin [41]. On a smaller scale it might be possible to use two-stage time location sampling, as the colleagues from Belgium did to reach a probability sample of misSA residing in Antwerp [42]. Using this approach they were also able to weight certain characteristics participants recruited at certain places might have exhibited. However, such a resource intensive approach would not have been feasible for a multicenter survey like ours. Instead, we asked peer researchers for their appraisal of which groups are the most important ones in the respective city and thus had to rely on their information on how their communities are comprised and where to reach missing groups for steering recruitment.
Conclusion
Working together with specifically selected peer researchers as a method of CBPHR and following a guided sampling procedure allowed us to conduct a survey on a sensitive topic among misSA living in Germany. In contrast to methods of probability sampling based on population registers, we were able to include especially hard-to-be-reached sub-groups like misSA with undocumented legal status or recent migrants, which is of particular importance for future prevention planning as these are particularly vulnerable for HIV transmission. For future CBPHR with misSA, peer researchers should be selected depending on the characteristics of participants researchers want to reach.
1 More recent data was not available when recruitment started.
References
- Robert Koch-Institut, HIV-Jahresbericht 2016. Epidemiologisches Bulletin, 2017. 39: p. 431-453.
- European Centre for Disease Prevention and Control and World Health Organization Regional Office for Europe, HIV/Aids surveillance in Europe 2017, 2016 data. 2017: Solna, Sweden & Copenhagen, Denmark.
- Zeitlmann N., et al., CD4-cell counts and presence of AIDS in HIV-positive patients entering specialized care—a comparison of migrant groups in the German ClinSurv HIV Cohort Study, 1999–2013. BMC infectious diseases, 2016. 16(1): p. 739.
- Hernando V., et al., HIV infection in migrant populations in the European Union and European Economic Area in 2007–2012: an epidemic on the move. JAIDS Journal of Acquired Immune Deficiency Syndromes, 2015. 70(2): p. 204-211.
- Wimmer-Puchinger B., H. Wolf and A. Engleder, Migrantinnen im Gesundheitssystem. Inanspruchnahme, Zugangsbarrieren und Strategien der Gesundheitsförderung. Bundesgesundheitsblatt, Gesundheitsforschung, Gesundheitsschutz,, 2006. 49(9).
- Norredam M., S. Nielsen and A. Krasnik, Migrants’ utilization of somatic healthcare services in Europe – a systematic review. European Journal of Public Health, 2010. 20(5).
- Suess A., et al., The right of access to health care for undocumented migrants: a revision of comparative analysis in the European context. European Journal of Public Health, 2014. 24(5).
- Prost A., A review of research among black African communities affected by HIV in the UK and Europe. University of Glasgow: Occasional Paper no. 15, Medical Research Council (MRC), Social and Public Health Science Unit. 2006: University of Glasgow: Glasgow, UK.
- European Centre for Disease Prevention and Control (ECDC),Technical Report: Mapping of HIV/STI behavioural surveillance in Europe. 2009, ECDC: Stockholm.
- Bundeszentrale für gesundheitliche Aufklärung (Hg.), AIDS im öffentlichen Bewusstsein der Bundesrepublik Deutschland 2011, Kurzbericht. 2012, BZgA: Köln.
- Statistisches Bundesamt (Destatis), Ausländer: Kreise, Stichtag, Geschlecht, Ländergruppierungen/Staatsangehörigkeit (12521-0041). 2016, Statistisches Bundesamt (Destatis): Wiesbaden.
- Statistisches Bundesamt (Destatis), Bevölkerung: Deutschland, Stichtag (12411-0001). 2016, Statistisches Bundesamt (Destatis): Wiesbaden.
- Treves-Kagan S., et al., Why increasing availability of ART is not enough: a rapid, community-based study on how HIV-related stigma impacts engagement to care in rural South Africa. BMC Public Health, 2016. 16(87).
- Chan BT. and AC. Tsai, HIV stigma trends in the general population during antiretroviral treatment expansion: analysis of 31 countries in sub-Saharan Africa, 2003-2013. Journal of acquired immune deficiency syndromes (1999), 2016. 72(5): p. 558-564.
- Fakoya I., et al., Barriers to HIV testing for migrant black Africans in Western Europe. HIV medicine, 2008. 9: p. 23-25.
- Prost A., et al., Social, behavioural, and intervention research among people of Sub-Saharan African origin living with HIV in the UK and Europe: literature review and recommendations for intervention. AIDS and Behavior, 2008. 12(2): p. 170-194.
- Manirankunda L., et al., “It’s better not to know”: perceived barriers to HIV voluntary counseling and testing among sub-Saharan African migrants in Belgium. AIDS Education & Prevention, 2009. 21(6): p. 582-593.
- Rommel A., C. Weilandt and J. Eckert, Gesundheitsmonitoring in der schweizerischen Migrationsbevölkerung. Endbericht. 2006, Wissenschaftliches Institut der Ärzte Deutschlands (WIAD) gem. e.V.: Bonn.
- International Collaboration for Participatory Health Research (ICPHR), Position Paper 1: What is Participatory Health Research? Version: May 2013. 2013, International Collaboration for Participatory Health Research: Berlin.
- von Unger H., et al., Training Immigrant Peer Researchers for CBPR on HIV/Aids in Germany, in CU Expo Conference 2011. 2011: Ontario, Canada.
- Dodds C., et al., BASS Line 2007 survey: Assessing the sexual HIV prevention needs of African people in England. 2008, Sigma Research: London, UK.
- Hickson F., et al., Bass Line 2008-09: assessing the sexual HIV prevention needs of African people in England. 2009, Sigma Research: Londom, UK.
- Gräser S., N. Krischke and C. Wohlrab, HIV/AIDS-Prävention und Versorgung für Migrantinnen und Migranten aus Sub-Sahara Afrika. Eine Pilotstudie zur Evaluation des ‚Afrika-Projekts’ des Gesundheitsamtes Bremen. Bremen: Schriftenreihe 03 des Institutes für Public Health und Pflegeforschung. 2009, Universität Bremen: Bremen.
- Gräser S., et al., MAQUA-HIV, Manual zur Qualitätssicherung in der HIV-Prävention für und mit MigrantInnen. 2013, Niebank-Rusch-Fachverlag: Bremen.
- von Unger H. and T. Gangarova, PaKoMi Handbuch: HIV-Prävention für und mit Migrant/inn/en. 2011, Deutsche AIDS-Hilfe e.V.: Berlin
- Ouedraogo OI., SF. Ouoguep and Wiebe M., Hand in Hand gemeinsam gegen AIDS. PaKoMi-Fallstudie Hamburg. Deutsch-Österreichischer AIDS-Kongress. 2011. Hannover
- Wright MT., M. Block and H. von Unger, Stufen der Partizipation in der Gesundheitsförderung: Ein Modell zur Beurteilung von Beteiligung. Infodienst für Gesundheitsförderung, 2007. 3: p. 4-5.
- von Unger H., et al., Stärkung von Gemeinschaften: Partizipative Forschung zu HIV Prävention mit Migrant/innen. Prävention und Gesundheitsförderung, 2013. 8(3): p. 10.
- von Unger H. Partizipative Gesundheitsforschung: Wer partizipiert woran. Forum Qualitative Sozialforschung, 2012. 13(1).
- Sadler KE., et al., Mayisha II Main Study Report: Assessing the Feasibility and Acceptability of Community Based Prevalence Surveys of HIV among Black Africans in England. 2005, Health Protection Agency: London, UK.
- Santos-Hövener C., et al., Determinants of HIV, viral hepatitis and STI prevention needs among African migrants in Germany; a cross-sectional survey on knowledge, attitudes, behaviors and practices. BMC Public Health, 2015. 15(1): p. 1-15.
- Statistisches Bundesamt (Destatis), Ausländer: Kreise, Stichtag, Geschlecht, Ländergruppierungen/Staatsangehörigkeit (12521-0041). 2013, Statistisches Bundesamt (Destatis): Wiesbaden.
- Santos-Hövener C., et al., Knowledge, Attitude, Behavior, and Practices Regarding HIV, Viral Hepatitis, and Sexually Transmitted Infections Among Migrants From Sub-Saharan Africa Living in Germany: A Multicenter Survey Protocol. JMIR Res Protoc, 2017. 6(5): p. e80.
- Santos-Hövener C., et al., Konzeption einer Studie zu sexueller Gesundheit bei in Deutschland lebenden Afrikanern. Prävention und Gesundheitsförderung, 2015. 10(1): p. 68-75.
- Kuehne A., et al., Impact of HIV knowledge and stigma on the uptake of HIV testing–Results from a community-based participatory research survey among migrants from sub-Saharan Africa in Germany. PloS one, 2018. 13(4): p. e0194244.
- Müllerschön J., Koschollek C., Santos-Hövener C., Kuehne A., Müller-Nordhorn J., Bremer V. (2019): Impact of health insurance status among migrants from sub-Saharan Africa on access to health care and HIV testing in Germany: a participatory cross-sectional survey. BMC International Health and Human Rights, 19:10.
- Koschollek C. and C. Santos-Hövener, Mapping afrikanischer Communities in Deutschland. Eine Analyse von Daten des Statistischen Bundesamtes. 2012, Robert Koch-Institut: Berlin.
- Simonson T., et al., Comportements face au VIH/sida parmi les migrants originaires d’Afrique subsaharienne en Suisse. 2015, Institut universitaire de médecine sociale et préventive – IUMSP, Centre d’évaluation et d’expertise en santé publique – CEESAN: Lausanne.
- Kastner B., Rassistischer Angriff auf Flüchtlings-Zelt, in Sueddeutsche Zeitung. 2015: München.
- Peter E., Geflüchtete in besetzter Schule: Sie wollen endlich ein normales Leben, in taz, die tageszeitung. 2017: Berlin.
- Salentin K. and H. Schmeets, Sampling immigrants in the Netherlands and Germany. Comparative Migration Studies, 2017. 5(21).
- Loos J., et al., TOGETHER Project to Increase Understanding of the HIV Epidemic Among sub-Saharan African Migrants: Protocol of Community-Based Participatory Mixed-Method Studies. JMIR Res Protoc, 2016. 5(1): p. e48.
-
Keywords
calibration CATI coverage coverage bias cross-national surveys data linkage data quality European Social Survey experiment face-to-face face-to-face survey Facebook hard to reach populations incentives item nonresponse measurement measurement error mixed-mode surveys multitasking non-probability samples Nonresponse nonresponse bias nonresponse rates paradata PIAAC Probability sample probability samples QR codes rare populations response rate Satisficing social desirability Social media survey survey-taking climate survey data survey management survey methods Telephone survey telephone surveys total survey error unit nonresponse validity web survey Web surveys weighting
